Warning! You are running svtsim lite with restricted functionality of svtsim for older Internet Explorer browsers (version 8 and older). Please upgrade to a modern browser!
In this tutorial, we explain the basis of electrophysiology studies (EPS) using svtsim software. svtsim is a a web-based cardiac electrophysiology study (EPS)/arrhythmia simulator, which is primarily designed for training and education. It provides an environment to simulate different cardiac arrhythmias and allows the user to perform various diagnostic maneuvers by pacing the simulated heart in realtime.
You should see seven simulated channels sweeping on a black surface: a surface ECG (corresponding to lead V1) and six simulated intracardiac electrograms recorded from virtual catheters located respectively at high right atrium (HRA), His location (His), proximal (CSp), middle (CSm) and distal (CSd) coronary sinus, and finally, the right ventricle apex (RV).
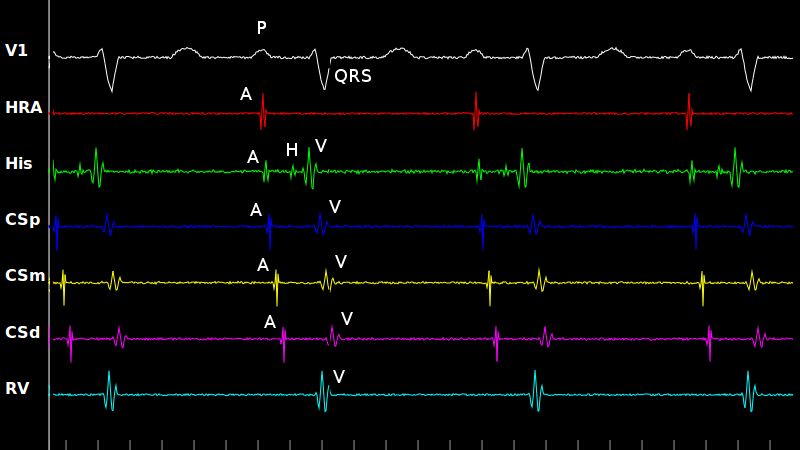
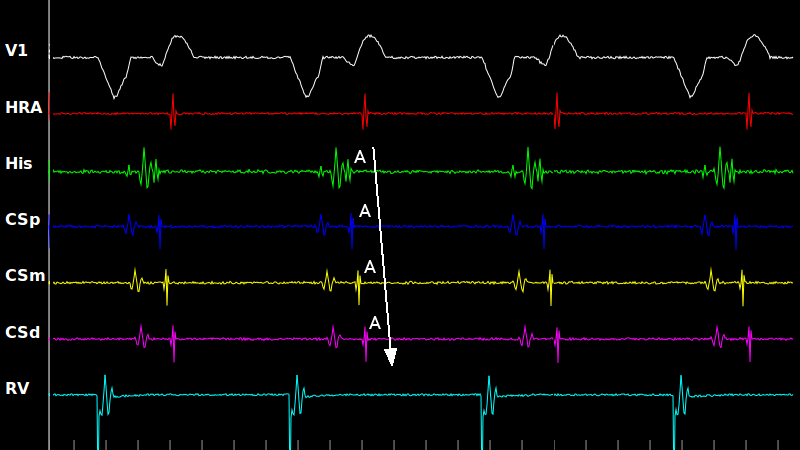
Let's look at a snapshot of the screen during normal sinus rhythm. Here, we have marked the signals in each channel. A cardiac cycle starts at the sinus node, which does not generate any visible signals on any surface or intracardiac channels. The first atrial signal is detected by the HRA catheter (marked A). Atrial activity propagates down to the His location, which is located centrally in the heart and records both the atrial (A) and ventricular (V) activities plus a small sharp signal from the His bundle (H) located in-between (A-H-V sequence). This strategic location of the His channel makes it very useful in recognition of the cardiac rhythm and various arrhythmias.
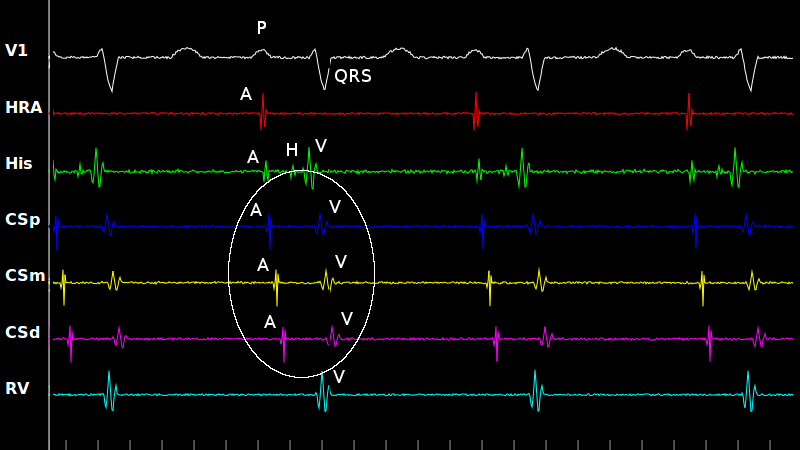
Coronary sinus catheter has multiple electrodes (see the white ellipse). In svtsim, we visualize three channels. The coronary sinus channels record both (left) atrial and ventricular signals. The atrial signals (A) are usually sharp, whereas the ventricular signals (V) are wider. In normal sinus rhythm, the atrial signal precedes the ventricular signal and both propagate from the proximal to the distal coronary sinus. This relationship may vary in different arrhythmias (especially those using an accessory pathway), as we will discuss later.
An Electrophysiology Study (EPS) begins with inspection of spontaneous rhythm and measurement of baseline intervals. In order to make a measurement in svtsim, you need to stop the signals by pressing the Pause button located on the left of the screen. When paused, a caliper is available. You can activate the caliper by pressing the left mouse button and dragging the mouse cursor to the desired location while holding the mouse button down. After a caliper is drawn, you may move or resize it by pressing near the horizontal (moving) or vertical (resizing) lines of the caliper and drag the mouse cursor to the new location. After the Pause button is pressed, it is renamed to Resume, which when pressed, resumes the sweeping.
Now, let's start our first practice. Look at the signals. They represent normal sinus rhythm. Pause and measure the baseline intervals: PP, RR, PR, AH and HV intervals. You can use the Select Interval drop-down list below the Pause button to help you with finding the right interval. PP, RR and PR are measured on the surface ECG channel. PP is the interval between two consecutive P waves in milliseconds. Similarly, RR is the interval between two consecutive R waves. AH and HV are measured on the His channel. There is also a VA interval option available from the drop-down list. It is usually not measured as part of the baseline EPS, but has an important role in the study of supraventricular tachycardias (SVT).
The normal value for PP and RR is 600-1000 ms (corresponding to a heart rate of 60-100 bpm). Normal PR, AH and HV intervals are 120-200 ms, 50-120 ms and 35-55 ms, respectively.
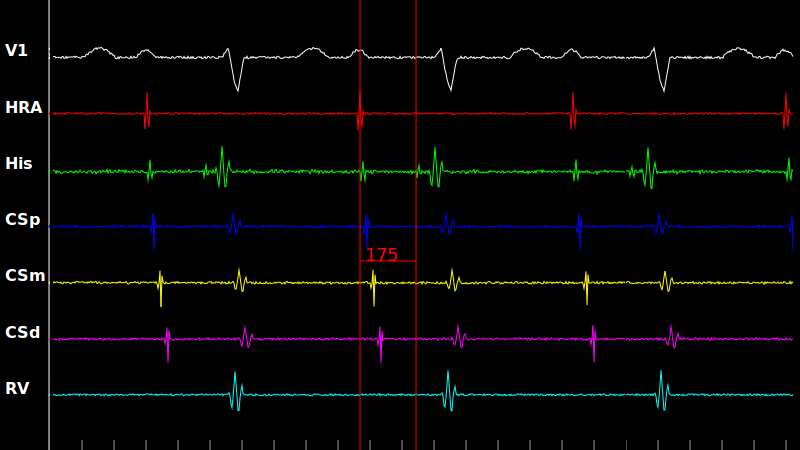
Measure the basic intervals in the case below. It shows first degree atrioventricular block. Where is the site of conduction delay?
In this snapshot of a case of first degree AV block, the caliper shows the AH interval. It is 175 ms, which is longer than the normal limits (50-120 ms). Therefore, slowing in conduction is in the AV node itself (nodal).
Of course the baseline rhythm might not be sinus. For example, we may encounter a tachycardia. This case shows a regular narrow complex tachycardia. It is in fact typical atrioventricular nodal reentrant tachycardia (AVNRT), but more on this later. Pause and measure the baseline intervals. Can you measure the VA interval? Use the Select Interval drop-down list for assistance.
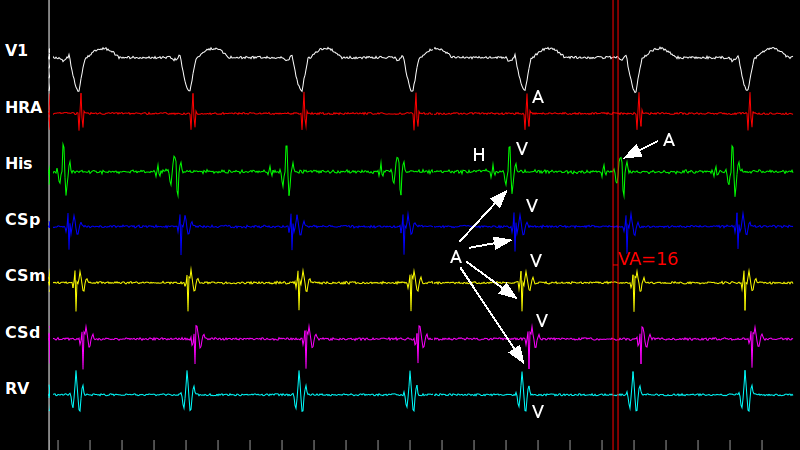
Let's look closer at the intervals during AVNRT. Note that the atrial signals is mostly fused with ventricular signals (specially in the His channel) and measuring the VA interval is, in fact, difficult. Sometimes, one needs to use clues from other channels to deduce where a given signal should be located on the channel of interest (e.g. we use the atrial signal in the coronary sinus channels to have a gross estimate of the atrial signal in the His channel).
The measured value of 16 ms is consistent with typical AVNRT, as we will discuss later.
Back to sinus rhythm. After inspection of the signals and measuring the baseline intervals, the bulk of an EPS is dedicated to performing Programmed Electrical Stimulation (PES) by pacing various locations inside the heart according to specific protocols. svtsim allows you to do a PES on the simulated heart with realistic response.
There are different types of PES, such as burst pacing, incremental pacing and delivery of extrastimulus (or stimuli). We explain each one in turn.
Burst Pacing is pacing at a fixed interval (in svtsim, burst pacing is also called straight pacing). By pressing Pace Straight button, you pace HRA at the interval specified in the S1 drop-down list until you press the button again.
One quantity that is measured using burst pacing is Sinus Nodal Recovery Time (SNRT). It is the interval between the last paced spike and the first return atrial signal on a surface or intracardiac channel and measures the sinus nodal function. Pace HRA at 600 ms for at least 10 seconds, stop pacing, pause after 1-2 seconds and measure the return interval. Hint: In this case, the p wave on the surface lead V1 in the earliest atrial activity.
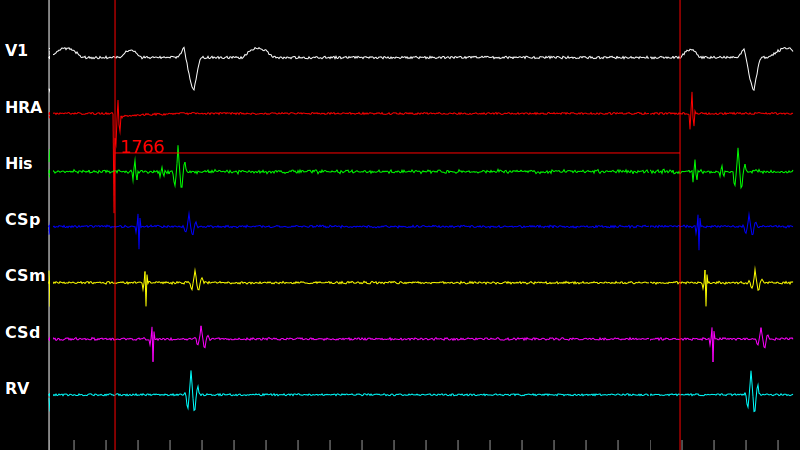
Now let's apply burst pacing to a case of sinus node disease (also known as sick sinus syndrome). Try the same protocol: pace HRA at 600 ms, stop pacing, pause after 2 seconds and measure the return interval. This time SNRT is much longer (see next slide).
The SNRT is measured around 1760 ms from the last stimulus to the first return atrial signal (p wave). We correct for the effect of heart rate on sinus nodal function by subtracting the basal cycle length (i.e. PP interval) from SNRT to calculate the Corrected Sinus Nodal Recovery Time (CSNRT). A normal CSNRT is below 500-550 ms.
In Incremental Pacing protocol, pacing starts at a pre-determined cycle length (similar to burst pacing), but the cycle length is gradually decreased until an expected event occurs. Note that the standard terminology is confusing, as we decrement the cycle length during incremental pacing (here incremental refers to the rate, not the cycle length). Incremental pacing is used to find the atrioventricular block cycle length (AVBCL), which is the longest cycle length for which 1:1 AV conduction is lost.
In order to perform incremental pacing in svtsim, you start by straight pacing and then decreasing the cycle length gradually by selecting a smaller number from the S1 drop-down list (or alternatively, by using the down arrow on the keyboard). Try to decrease the cycle length by 10 ms every 3-4 beats. What is AVBCL in this case (see next slide)?
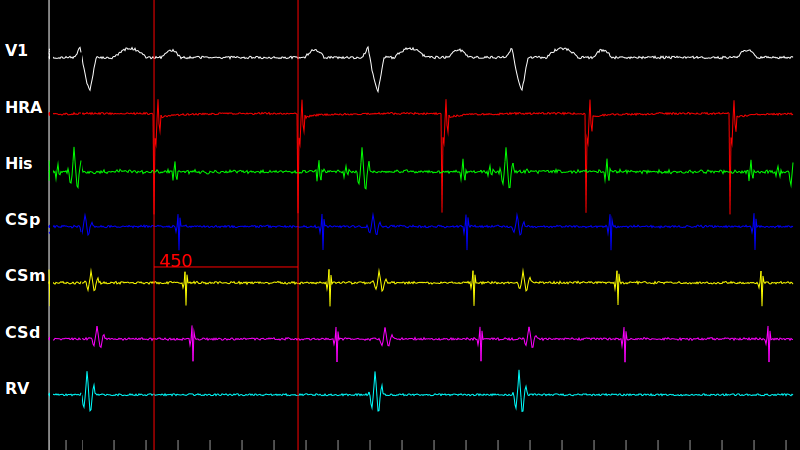
This is a snapshot from the protocol in the previous slide. Note the AV block (dropped QRS complexes and ventricular signals) while pacing at a cycle length of 450 ms. Therefore, AVBCL is 450 ms (since there is no block at a higher cycle length).
During EPS, it is very important to determine the level of AV block (nodal vs infranodal). Nodal means that block occurs at the level of the AV node, which is generally benign and does not need pacemaker implantation. Infranodal block usually implies a diffuse disease in the cardiac conduction system and can be an indication for pacemaker.
Presence of His signal in a beat with blocked QRS is characteristics of infranodal block. Try it by performing incremental pacing until 1:1 AV conduction is lost and then pause. Look for a His signal in the blocked beats. Is it present?
The case in the previous slide represented Wenckebach (or Mobitz type I) second degree AV block. There was no His signal in the blocked beats and the level of block was nodal. Let's try the same incremental pacing protocol to a case of infranodal block. Do you remember the protocol? Pace straight, decrease the cycle length by 10 ms every 3-4 beats until loss of 1:1 AV conduction and pause. Do you see the His signal now (see next slide)?
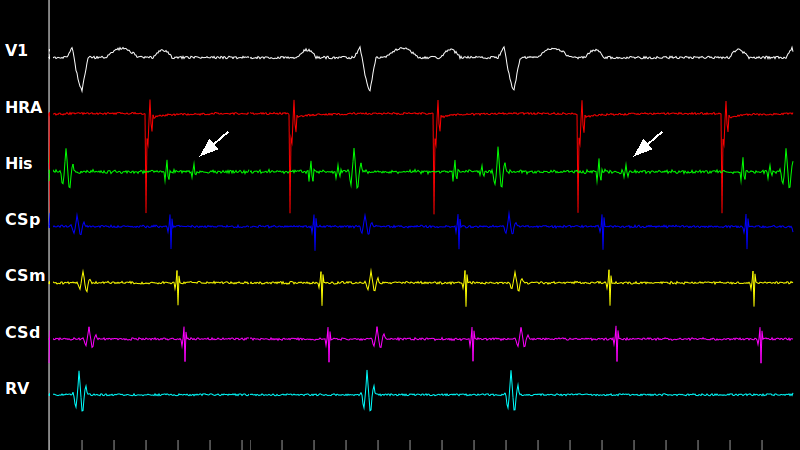
Now, a His signal (arrows) is present in the blocked beats. This means that the activation has crossed the AV node and has reached the His bundle, but has not propagated to the ventricles. In other word, the block level is between the His bundle and ventricles (infranodal block).
Up to this point, we have only paced from HRA channel. Here, we practice incremental RV pacing to check for ventriculoatrial block cycle length (VABCL).
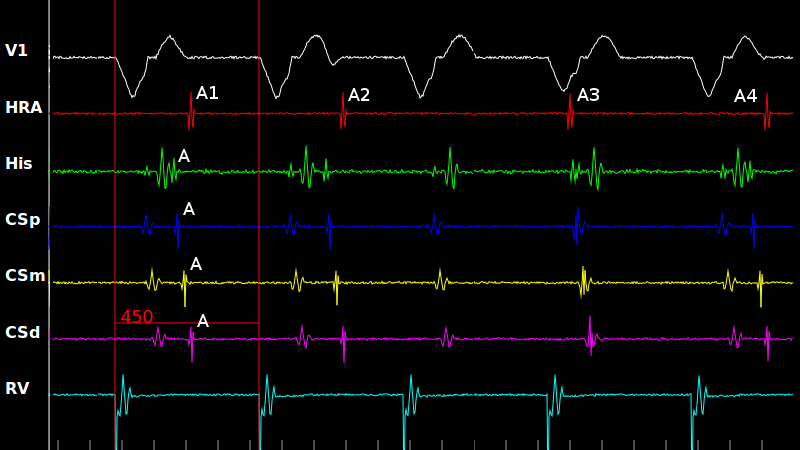
Let's inspect the ventricular pacing protocol in more detail. In this snapshot, the first two ventricular paced complexes conduct retrogradely generating atrial signals A1 and A2. The expected third retrograde A does not occur (it is blocked in the AV node), therefore VABCL is equal to the pacing cycle length at this time (450 ms). However, the next observed atrial signal (A3) comes earlier than expected. It is in fact a sinus (escape) beat and not a retrogradely conducted beat. A4 is again retrograde similar to A1 and A2. Also note that to claim that VABCL is 450 ms requires that there is no block at a higher cycle length. This is the case here, since there was no block pacing at 460 ms.
Another important observation during ventricular pacing is the atrial activation pattern. Pace RV at 600 ms (burst pacing) and look at the atrial activation. We will review the result in the next slide, but first try to figure the order in which atrial signals propagate.
Hint: If you have difficulty finding the atrial signal in the His channel (in might be fused with the ventricular signal), select AH interval from the Select Intervals drop-down list. It points you to the atrial signal.
Let's review! Note that the first atrial signal occurs in the His channel and the activation is from proximal to distal in the coronary sinus channels (arrow). This is called concentric atrial activation and is the normal pattern.
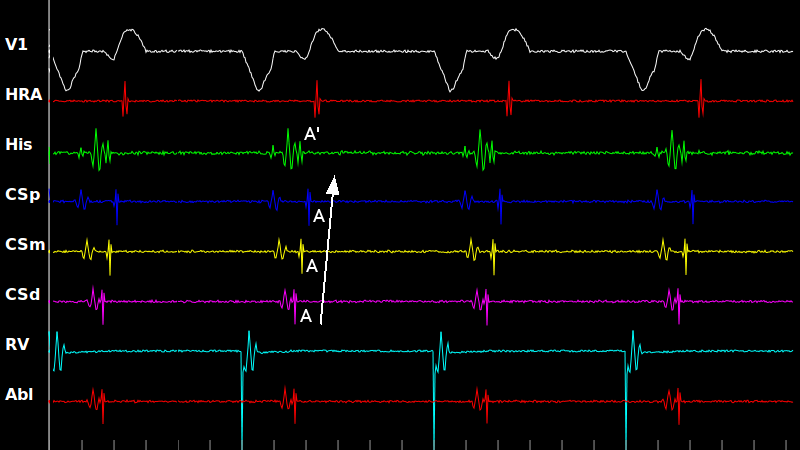
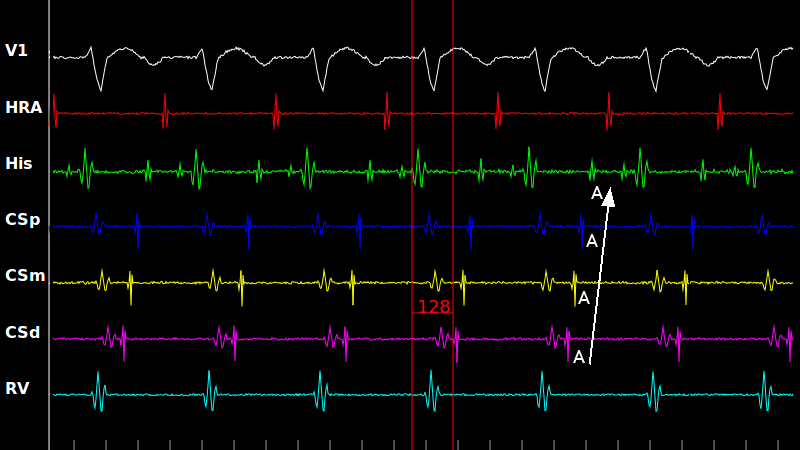
Now we discuss the eccentric activation. In this case, there is a concealed lateral accessory pathway. It means there is a connection between ventricle and distal coronary sinus that conducts only from the ventricle to the atrium (no antegrade conduction, only retrograde conduction). Pace RV and observe the atrial activation pattern.
Note that during the eccentric activation, the first atrial signal occurs at CSd channel (distal coronary sinus), then the activation propagates to the middle and proximal coronary sinus (arrow). However, also note that the His catheter records an atrial signal (A') before proximal coronary sinus. How can this happen? It means that the retrograde conduction is via both the accessory pathway (hence the eccentric activation) and through the AV node. This combination of two activation patterns is an example of the fusion phenomenon. As we will see later, during orthodromic reciprocating tachycardia (WPW tachycardia) using a lateral accessory pathway, the atrial activation pattern is purely eccentric.
Back to sinus rhythm and atrial pacing. After practicing the burst and incremental pacing methods, it is time to discuss the Extrastimuli Pacing protocol. It consists of a drive train of 6-10 paced beats at a fixed cycle length (similar to burst pacing), followed by one or more paced beats at shorter intervals. We use the terminology of calling the drive train cycle length S1 and the coupling interval between the last beat in the drive train and the first extrastimulus S2 (S3 and S4 are defined similarly if applicable).
Delivery of extrastimuli has two main applications: measuring refractory periods and inducing arrhythmias. The effective refractory period (ERP) of a tissue is the longest coupling interval for which a premature impulse fails to propagate through that tissue (definition from Fogoros).
Let's measure the atrioventricular effective refractory period (AVERP). Note that now there is a S2 drop-down list in addition to S1. The protocol is to pace HRA at a drive train of 600 ms (S1) and then deliver a single extrastimulus, starting from a coupling interval (S2) of 500 ms and decrease it by 10 ms at every run. Press Pace & Pause button. Note that the signals pause automatically after the delivery of S2 to assist with measurements. Decrease S2 by 10 ms, resume and then press Pace & Pause for the next run. Repeat until the extrastimulus fails to propagate through the AV node (no QRS complex). Now, S2 is equal to AVERP.
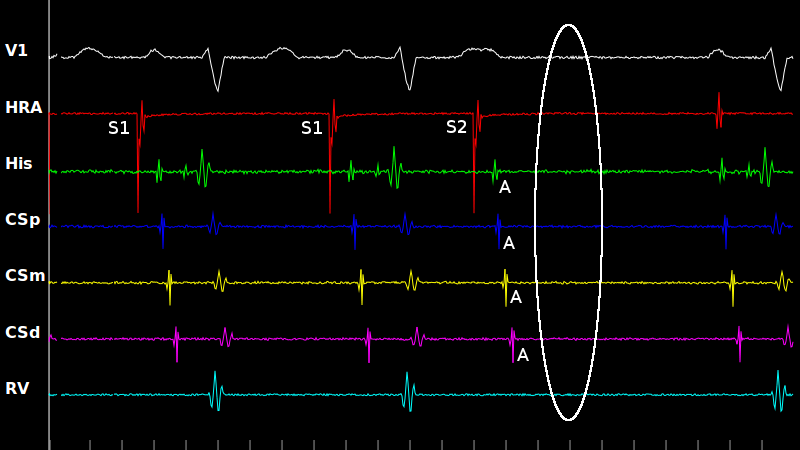
This is a snapshot after delivery of an extrastimulus that blocks in the AV node. We have marked The paced beats: S1 for the beats in the drive train and S2 for the extrastimulus. Note that S2 generates atrial activity (A) but no His signal or ventricular activities (the ellipse shows the location of the expected, but missing, ventricular signals).
Let's practice the extrastimuli protocol more. Remember, press Pace & Pause button, wait until paused, decrease S2 by 10 ms, resume and then press Pace & Pause for the next run. Repeat until the extrastimulus fails to propagate (no QRS complex). Note that in this case, there is a His signal at the time of block. This means that the block is infranodal. To find the true atrioventricular nodal effective refractory period (AVNERP rather than AVERP), you need to continue the protocol until His signal vanishes too. Hint: In the current case, there is a large gap between AVERP and AVNERP.
The extrastimuli protocol is not limited to HRA pacing. We can find the ventriculoatrial ERP (VAERP) by performing a similar protocol (pace, pause, decrement, resume, and repeat).
All the previous examples of measuring the refractory period deal with AVERP. The refractory period can also be measured for other cardiac tissues, such as the atrial refractory period (AERP) and ventricular refractory period (VERP). These parameters are rarely measured during a basic EPS; however, there are certain conditions where they need to be obtained. Another clinically important parameter is the antegrade refractory period of an accessory pathway in Wolff-Parkinson-White (WPW) syndrome, which will be explained in details in another tutorial.
Now, we spend some time on the crucial concept of dual AV nodal physiology, which is central to the mechanism of AVNRT. In 10-15% of population, the AV node is conceptually consist of two parallel pathways with different refractory periods and conduction delays. The fast pathway has a longer refractory period, but faster conduction. The slow pathway has shorter refractory period, but slower conduction. Note that the AV node (including the fast and slow pathways) is responsible for the AH interval.
When we perform the extrastimuli protocol in a case of dual AV nodal physiology, the fast pathway has a longer refractory period and blocks first. When this happens, the conduction through the AV node shifts from the fast to the slow pathway. Since the slow pathway is slower, the AH interval prolongs at the fast pathway ERP. This is called a jump and is the signature of dual nodal physiology. The jump is formally defined as an increase of at least 50 ms in AH after a 10 ms decrement in S2 coupling interval. What are the fast and slow pathways ERP in this case?
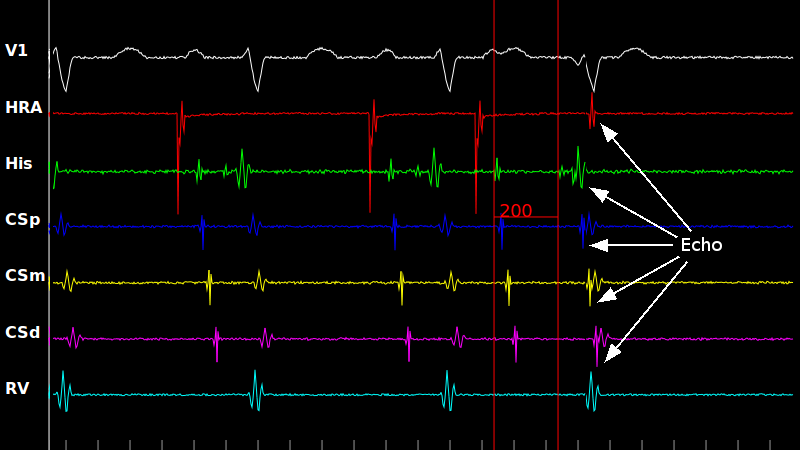
Let's look closer at the time when the fast pathway blocks (the pace setting is S1=600 ms and S2=330 ms). There is a jump in AV nodal conduction (AH prolongs to 200 ms). However, also note that there is atrial activity around the same time as the QRS complex generated by S2. This is an example of an echo beat (arrows point to the atrial signal). What happens is that after the fast pathway blocks, the activation propagates down the slow pathway. By the time the activation reaches the end of the slow pathway, enough time has passed that the fast pathway is out of refractoriness. Therefore, the fast pathway is activated retrogradely and the activation returns to atria.
As we mentioned before, 10-15% of population have dual AV nodal physiology. Most of them never have any arrhythmias as a result of dual nodal physiology. However, there is a small group of patients who can sustain reentrant activity, which is in fact back-to-back echo beats. Try it yourself in this case! Perform an extrastimuli pacing protocol until the fast pathway blocks. What happens?
You can terminate the tachycardia by pressing the Cardiovert button or you can try to break the tachycardia by rapid atrial pacing (set S2=0 and use S1 to deliver burst pacing). Hint: You need to pace much faster than the tachycardia cycle length to terminate it.
Induce tachycardia in this AVNRT model as before. Look at the relationship between the atrial and ventricular activation (measure VA). This is an example of short RP tachycardia, i.e. the interval from a QRS complex during tachycardia to the next p wave (RP) is shorter than the interval from a p wave to the next QRS complex (PR). The three main short RP tachycardias are typical AVNRT, orthodromic reciprocating tachycardia using an accessory pathway (WPW syndrome) and atrial tachycardias.
Let's look at another tachycardia. Do you see the difference from AVNRT? Hint: Observe the atrial activation pattern and measure the VA interval. Is atrial activation concentric or eccentric? What is the mechanism of tachycardia?
This is an example of ORT (WPW-related tachycardia) using a lateral accessory pathway. The atrial activation pattern is eccentric (note atrial signal on the His channel, this is a pure eccentric pattern, not a fused as shown before during ventricular pacing). The VA time (shown by the calipers) is relatively long (more than 70 ms), whereas it is usually less than 70 is AVNRT.
We will discuss induction, recognition and ablation of supraventricular tachycardias in separate tutorials. The planned advanced tutorials are:
EPS 201: Basic Diagnostic Maneuvers in Supraventricular Tachycardias
EPS 301: Advanced Diagnostic Maneuvers in Supraventricular Tachycardias
EPS 302: Atrial Fluter
Snapshot
S1:x 8
S2:
svtsim is a web-based cardiac electrophysiology study (EPS)/arrhythmia simulator, which is primarily designed for training and education. Its target audience includes cardiology and clinical cardiac electrophysiology fellows-in-training and electrophysiology laboratory nurses and technicians. svtsim provides an environment to simulate different cardiac arrhythmias. It allows the user to perform various diagnostic maneuvers by pacing the simulated heart in realtime.